
Back to Blog

Flexor Hallucis Longus: FHL, Muscle of the Day
Seeing as the last anatomical post that I had took quite awhile to write out, I’m going to make things a little more manageable by giving some nice in-depth info about a single muscle that you may not know you have (rather than going through the layers of the shoulder!)
Today: The FHL or flexor hallucis longus. Hallucis or hallux is another term for your big toe (the reason they sometimes call bunions hallux valgus/rigidus), flexor because it flexes the toe, and longus (lt: long) to differentiate it from brevis (lt: short).
Anatomy
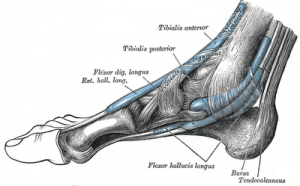
The FHL starts in the posterior calf as one of the deepest muscles, attaching it’s muscular contractile unit to the posterior fibula (mid-level) and spans down the calf. The distal attachment of the tendon is to the inferior (plantar) distal phalanx of the great toe (hallux). From start to finish, this tendon makes its way through 2 narrow gateways:
- The fibro-osseus tunnel behind the medial malleolus (inside heel bone point)
- The tunnel between the small circular seasmoid bones of the FHB (flexor hallucis brevis)
The tibial nerve (a section of the great sciatic) is what innervates the FHL.
Action
If you picture where the FHL runs to and from, you can see how this muscle will plantarflex the toe in a non-weight bearing position (in addition it will plantarflex the ankle – but very weakly). In weight-bearing, the muscle is active through mid-stance, supporting and slowing the ankle segment through motion.
Pathology
When does this become a problem? If you are a dancer that spends some time doing jumping and landing (particularly ballet) there is a good chance you’ve already had an issue with the FHL. Another sport that can have issues with this are those who run on hard surfaces with poor shoe support (think: soccer on hard ground or sprinters on cement). A recent case study was on a 42 year old male client with FHL irritation during racquetball.
Injury can happen from the constant friction through the aforementioned gateways, or by muscular overuse (especially if there is a decreased activation of other plantarflexors of the ankle!).
Deep pain in the posterior calf, behind the medial malleolus, or a the bottom of the foot. Sometimes it can appear as a calf irritation, or even plantar fasciitis, though without specific treatment to the FHL, rehab would likely be poor.
Proper diagnosis by your physiotherapist is extremely important, especially since this issue can mimic other injuries. Treatments should include assessment of footwear and possible addition of metatarsal pad or arch support, as well as manual myofascial release of the FHL and manual stretching. Ultrasound may have some benefit especially during the early stages to help with swelling.
Howard, P.D. (2000) Differential Diagnosis of Calf Pain and Weakness: Flexor Hallucis Longus Strain. Journal of Orthopaedic & Sports Physical Therapy 30(2). pp. 78-84.
Travell, J.G., & Simons, D.G. (1993). Myofascial Pain and Dysfunction: The Trigger Point Manual, The Lower Extremity (VOl 2). Philadelphia: Lippincott Williams & Wilkins.